https://diotima.dingherself.com/handouts/fausto-sterling.htmlDing
Anne Fausto-Sterling, Sexing the Body
Posted: Mon, Mar 9, 2026
Today
- Beauvoir the political lesbian?? [20 min]
- Sexing genitalia [45 min]
- More questions about the first paper? [save 10 min]
Intersex people
“Sex assignment at birth” is not a metaphor or euphemism.
Fausto-Sterling’s estimate: 1.728 in 100
Some examples:
- Congenital Adrenal Hyperplasia (CAH): in XX children, masculine-appearing genitalia
- Note already the language we use to describe this: “For instance, the clitoris may be enlarged and resemble a penis. The labia may be partly closed and look like a scrotum. The tube through which urine leaves the body and the vagina may be one opening instead of two separate openings.” (Mayo Clinic)
- Androgen Insensitivity Syndrome (AIS): in XY children, female-typical genitalia
- Turner Syndrome: 45,X0
- Klinefelter Syndrome: 47,XXY
- Jacobs Syndrome: 47,XYY
- Trisomy X: 47,XXX
- … and more
- PCOS? (debated)
Nomenclature: Disorders of Sex Development (DSD) vs. intersex variations
Traditional model for managing intersex newborns
Background: John Money’s gender identity theory
Recall David Reimer from the documentary: The “John/Joan” case.
- Gender identity: One’s sense of oneself as gendered one way or another.
- Gender identity is not a biological given: we are not born with it.
- Rather, it is learned and developed through socialization.
- Gender identity is highly malleable during early childhood.
- Gender identity need not align with genitalia, sex hormones, or sex chromosomes.
Assumptions of the traditional model
- Sex is a clear-cut division between males and females.
- Those born with “ambiguous” genitalia have a true sex waiting to be discovered by science.
- It is medically urgent that the ambiguity be surgically “fixed” early on.
- While some physicians now support limited transparency, this is a very recent development.
Why the urgency?
Parents
“Even though genderidentity theory places the critical age limit for gender reassignment between eighteen months and two years, the physician acknowledge that diagnosis, gender assignment, and genital reconstruction cannot be delayed for as long as two years, since a clear gender assignment and correctly formed genitals will determine the kind of interactions parents will have with the child. The geneticist argued that when parents ‘change a diaper and see genitalia that don’t mean much in terms of gender assignment, I think it prolongs the negative response to the baby. . . . If you have clitoral enlargement that is so extraordinary that the parents can’t distinguish between male and female, it is sometimes helpful to re-duce that somewhat so that the parent views the child as female.’ Another physician concurred: parents ‘need to go home and do their job as child rearers with it very clear whether it’s a boy or a girl.’” (Suzanne Kessler, “The Medical Construction of Gender,” 1990, p. 9)
Gender identity development
Fausto-Sterling reports that many physicians “emphasiz[e] that nuanced scientific understanding of anatomical sex is incompatible with a patient’s need for clear-cut gender identity.”
- On Money’s theory, if surgical interventions are completed in time, intersex children will come to develop gender identities that align with the sex surgically assigned to them.
- But Money’s theory has been debunked by David Reimer’s case.
Sexual orientation development
With successful surgical interventions, intersex children will develop “appropriate” partner and sexual preference (i.e., PIVI).
Trauma of castration
Kessler writes,
Money suggests that if reduction of phallic tissue were delayed beyond the neonatal period, the infant would have traumatic memories of having been castrated. . . . Although physicians speculate about the possible trauma of an early childhood ‘castration’ memory, there is no corresponding concern that vaginal reconstructive surgery delayed beyond the neonatal period is traumatic. (pp. 8–9)
Why not full transparency?
- Parents are usually told that their child has “underdeveloped” genitalia, as if all that needs to be done is to let the genitalia grow just a little bit more and the child will reveal themself as either female or male.
- Information is also usually (partially or fully) withheld from intersex children themselves, even when they grow up. “An intersex child assigned to become a girl, for instance, should understand any surgery she has undergone not as an operation that changed her into a girl, but as a procedure that removed parts that didn’t belong to her as a girl.”
Why? Pp. 64–65.
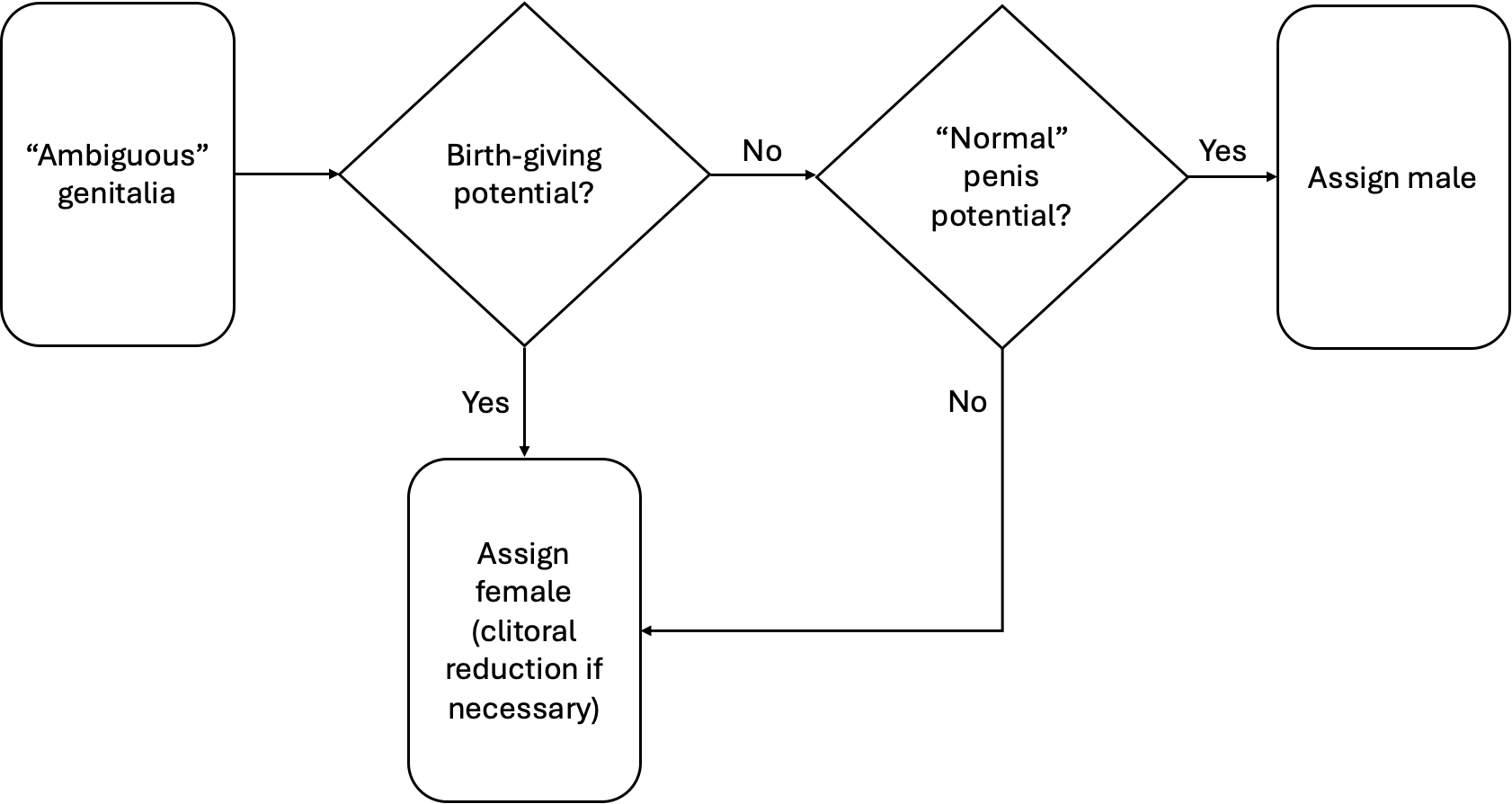
So, how do you determine the “true sex”?
Patricia Donahoe’s recommendations are highly illustrative: “Genetic females should always be raised as females, preserving reproductive potential, regardless of how severely the patients are virilized. In the genetic male, however, the gender of assignment is based on the infant’s anatomy, predominantly the size of the phallus” (p. 57).
- The “standing up to pee” test: “Young boys should be able to pee standing up and thus to ‘feel normal’ during little-boy peeing contests.”
- The “vaginal penetration” test: “[A]dult men, meanwhile, need a penis big enough for vaginal penetration during sexual intercourse.”
- The Phall-O-Meter ®
Some more recent developments
- In July 2020, Lurie’s Children Hospital in Chicago became the first U.S. hospital to apologize for performing intersex surgeries.
- A few months later, Boston Children’s Hospital also announced that it “will not perform clitoroplasty or vaginoplasty in patients who are too young to participate in a meaningful discussion of the implications of these surgeries, unless anatomical differences threaten the physical health of the child.”
- In July 2021, New York City Health & Hospitals announced that they would defer all unnecessary intersex surgeries until the child is old enough to meaningfully participate in a decision.
The medical construction of the American family
Project 2025:
The Secretary [of Health and Human Services] should pursue a robust agenda to protect the fundamental right to life, protect conscience rights, and uphold bodily integrity rooted in biological realities, not ideology. . . .
Radical actors inside and outside government are promoting harmful identity politics that replaces biological sex with subjective notions of “gender identity” and bases a person’s worth on his or her race, sex, or other identities. This destructive dogma, under the guise of “equity,” threatens American’s fundamental liberties as well as the health and well-being of children and adults alike. The next Secretary must ensure that HHS programs protect children’s minds and bodies and that HHS programs respect parents’ basic right to direct the upbringing, education, and care of their children. (p. 450)
Executive Order 14168: Defending Women from Gender Ideology Extremism and Restoring Biological Truth to the Federal Government
Across the country, ideologues who deny the biological reality of sex have increasingly used legal and other socially coercive means to permit men to self-identify as women and gain access to intimate single-sex spaces and activities designed for women, from women’s domestic abuse shelters to women’s workplace showers. This is wrong. Efforts to eradicate the biological reality of sex fundamentally attack women by depriving them of their dignity, safety, and well-being. The erasure of sex in language and policy has a corrosive impact not just on women but on the validity of the entire American system. Basing Federal policy on truth is critical to scientific inquiry, public safety, morale, and trust in government itself.
This unhealthy road is paved by an ongoing and purposeful attack against the ordinary and longstanding use and understanding of biological and scientific terms, replacing the immutable biological reality of sex with an internal, fluid, and subjective sense of self unmoored from biological facts. Invalidating the true and biological category of “woman” improperly transforms laws and policies designed to protect sex-based opportunities into laws and policies that undermine them, replacing longstanding, cherished legal rights and values with an identity-based, inchoate social concept.
Some notable points for discussion:
- “Gender identity” is not a new ameliorative conceptual framework to expand gender equality rights; it is deeply rooted in a pathologizing sexology of the 50s and 60s.
- What is actually the biological reality, and what is perniciously ideological?
- It seems true that “the validity of the entire American system” depends on a particicular ideological misrepresentation—and surgical alteration—of biological reality!